Improving Atrial Fibrillation Diagnosis and Treatment
by Adrienne Mueller, PhD
January 5, 2023
Heart rhythm disorders be extremely debilitating, even leading to heart failure or stroke. Atrial fibrillation - an irregular and often very fast heartbeat - is the most common heart rhythm disorder. It affects approximately 1% of the population overall, and 10% of people over the age of 70. A subset of individuals with atrial fibrillation transition to a condition called atrial tachycardia, with an abnormally fast heart rhythm. It is possible to treat atrial fibrillation and atrial tachycardia by removing a small part of the patient’s heart tissue that is functioning abnormally and contributing to the rhythm disorder. The success rate of this surgical intervention is 50-70%: sometimes patients with these conditions respond to removal of part of their heart tissue, but sometimes they do not. It’s unclear why the treatment is more likely to be effective in some patients than others.
In a recent study published in Europace, a team of investigators led by Prasanth Ganesan, PhD, and Sanjiv Narayan, MD, PhD, tested the hypothesis that the size (area) of the region that shows the organized (normal) activity correlates with a spectrum of responses: from atrial tachycardia that responds very well to treatment by ablation (cautery), to atrial fibrillation which responds to treatment, to atrial fibrillation which does not respond.
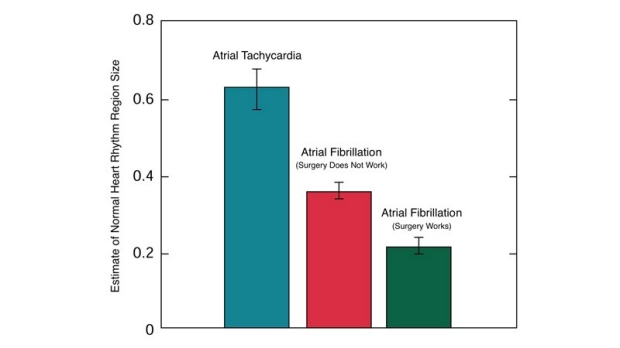
The size of the abnormal is correlated with a spectrum of atrial fibrillation to atrial tachycardia symptoms.
The investigators studied 150 patients and found heart regions with normal measured activity were largest in patients with atrial tachycardia (i.e. least abnormal), smaller in atrial fibrillation patients for whom the surgery worked, and smallest ‘normal’ regions in patients for whom the surgery had no effect.
This study showed that the size of area of abnormal activity in the atrial chamber of the heart can determine the type of heart rhythm defect a patient experiences: ranging from atrial tachycardia to atrial fibrillation that will respond to surgery to atrial fibrillation that will not respond to surgery. Future studies will be able to use this information to improve diagnosis and treatment in patients with heart rhythm disorders during a procedure.
Additional Stanford Cardiovascular Institute-affiliated investigators who contributed to this study include Brototo Deb, Ruibin Feng, Albert J Rogers, Paul Clopton, and Paul J Wang.

Prasanth Ganesan, PhD

Sanjiv Narayan, MD, PhD