Unraveling the Mystery of Immune Checkpoint Inhibitor Myocarditis
by Amanda Chase, PhD
September 2, 2022
Our immune system acts in a tightly regulated way to maintain our health. Components of the immune system recognize self vs non-self (e.g., virus, bacteria, cancer cell) by immunosurveillance and orchestrate a response to clear the body of “non-self”. Importantly, there are also mechanisms (immune checkpoints) to stop the immune response from being too robust and destroying healthy cells. Unfortunately, this system is not fail-proof. Cancer cells in a tumor, for example, can change what is shown on their surface (major histocompatibility molecules) to avoid detection by immunosurveillance. These tumor cancer cells can also create more proteins on their surface that are recognized and bound by T immune cells (T cells) to create an “off” signal for the T cells. This creates an immune checkpoint that turns off the T cell response to protect the cancer cell.
It is known that major immune checkpoints include the programed cell death 1 (PD-1) and cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) pathways. From that, revolutionary checkpoint inhibitor (ICI) therapies were created to treat cancers. ICIs block the interaction between the checkpoint protein (CTLA-4 or PD-1) and their binding partner to allow T cells to recognize and destroy the cancer cells. While ICIs have been instrumental in improving life expectancy of cancer patients, they are also associated with immune related adverse events (irAE). One such side effect is myocarditis, with up to 50% mortality in affected patients and leading to significant long-term complications such as arrhythmias and heart failure. Despite the high mortality rate of ICI-induced myocarditis, very little is understood.
Given both the severity of myocarditis and the necessity for patients to receive ICI therapy, there is a critical need to quickly and accurately diagnosis ICI-induced myocarditis and to decide whether to discontinue ICI therapy and treat with immunosuppressants to minimize cardiac morbidity. Researchers from Stanford Cardiovascular Institute, led by Han Zhu and senior authors Patricia Nguyen and Sean Wu, recently started to address this critical need. Their findings, published in Circulation, present novel potential disease biomarkers of ICI myocarditis and candidate therapeutic targets in the prevention and treatment of ICI myocarditis. Researchers used complementary approaches to create the first comprehensive profile of blood mononuclear cells (drivers of immune response) of patients with ICI myocarditis to understand how the cells were unique from immune cells in healthy individuals and in ICI-treated patients without myocarditis. Interestingly, they found a unique population of immune cells (CD8+ T-cells expressing CD45RA; Temra) in patients with ICI myocarditis, compared to ICI-treated patients without any immune related adverse effects or those with non-cardiac immune related adverse effects. Additional confirmatory studies in a PD-1 deficient mouse model of myocarditis suggest that these unique immune cells may be found specifically in the heart.
This study by Zhu and colleagues showed that the special immune cells (Temra CD8+) are critically associated with ICI myocarditis. Temra CD8+ cells may, therefore, be a disease biomarker of ICI myocarditis for aiding the difficult decision to discontinue ICI therapy to minimize cardiac morbidity and mortality. Additionally, finding chemokines—molecules that help direct immune cells to areas of inflammation—that are expressed in the heart by Temra CD8+ cells provide potential therapeutic targets in the treatment of ICI myocarditis, as well as other types of heart inflammation. Together, these findings have significant potential for improving the cardiovascular safety of cancer patients treated with ICI therapy.
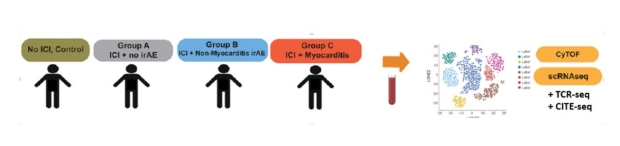
Blood mononuclear cells were collected from healthy control, ICI-treated patients without adverse immune response (Group A), with non-myocarditis adverse immune response (Group B), and with myocarditis (Group C). Complementary approaches (CyTOF, scRNAseq, etc) were used to understand how these cells were unique. A special immune cell subset (Temra CD8+) was found to be preferentially associated with ICI myocarditis.
Other Stanford Cardiovascular Institute authors include Francisco Galdos, Daniel Lee, and Julia Ryan. Stanford University researchers include Sarah Waliany, Joel Neal, Heather Wakelee, Sunil Reddy, Sandy Srinivas, Lih-Ling Lin, Ronald Witteles, Holden Maecker, and Mark Davis. Work was also done in collaboration with Cornell University (Yuhsin Huang) and University of California, Santa Barbara (Katherine Dang).
Han Zhu, MD

Patricia Nguyen, MD

Sean Wu, MD, PhD