Understanding that Different Leaflets Have Different Effects in Calcific Aortic Stenosis
by Amanda Chase, PhD
March 3, 2022
The heart functions in a highly regulated manner to facilitate blood flow through the body. The heart itself is composed of four chambers that are connected by heart valves between the chambers. Imagine the chambers as rooms in the heart and the valves as the doors between the rooms. The opening and closing of the valves, or doors, allows the correct amount of blood to flow from one chamber to the other. Each valve is made up of flaps, or leaflets (cusps), that open and close to control blood flow. When affected by disease, valves can stop opening fully to result in reduced blood flow. When this occurs on the aortic valve, which is normally composed of three leaflets, the area through which blood moves out of the heart to the body is then narrowed; this is called aortic stenosis (AS). Patients with this condition can experience dizzy spells and chest pain because of reduced blood flow to the brain and the heart itself. They can also develop heart failure because of the extra work that the heart must perform to pump blood through a narrowed valve.
There are different causes of AS. The most common cause in the Western world is due to increased deposition of calcium on the aortic valve (calcific AS). Although calcific AS used to be thought of as a disease of “wear and tear,” more recent studies suggest that calcification of the aortic valve results from active biological processes within the valve that mimic, to some extent, how bone is formed in the body. AS is typically confirmed, and severity determined, by an echocardiogram that uses ultrasound to image your heart in motion. Clinicians can use it to monitor the progression of AS. When the echocardiographic results are not clear, a computerized tomography (CT) scan that uses X-ray to create cross-section views of the heart can also be used to confirm the severity of AS based on the extent of aortic valve calcification. Calcific AS is a progressive disease without effective drug treatments. Most patients with this condition will eventually need surgery, if they live long enough, to replace the diseased aortic valve. The use of echocardiography and CT scans can help guide the timing of valve replacement.
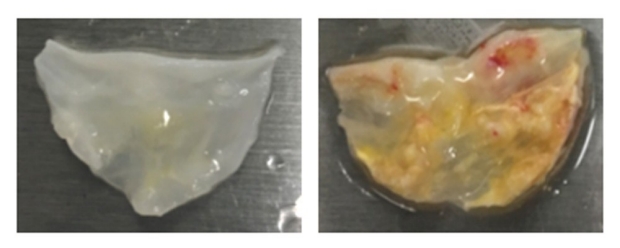
Figure. Healthy leaflet (left) versus diseased leaflet (right).
Interestingly, it has been frequently seen in clinic that patients with calcific AS can have significant differences in calcium build-up among the leaflets of the same valve. This suggests that, contrary to popular belief, not all leaflets behave the same or are subject to the same levels (or types) of stress. The functional implications of this observation could be important for understanding how AS progresses.
In a recent study published in Circulation: Cardiovascular Imaging, researchers looked back at CT scans (CT angiograms) from patients with calcific AS to see if there were any differences in calcium build-up, in relation to leaflet appearance and mobility, among different leaflets of the aortic valve. The team was led by first authors Ian Chen (Stanford Cardiovascular Institute, Veterans Affairs Palo Alto Health Care System) and Vijay Vedula (now at Columbia University) and senior authors Joseph Wu (Director of the Stanford Cardiovascular Institute) and Alison Marsden (Stanford Cardiovascular Institute). They looked at CT scans that had been previously obtained for 200 male patients undergoing evaluation for valve replacement because of calcific AS, as well as 20 male control patients who had normal aortic valves. Using a combination of image analysis and computer simulation techniques, the team showed that in patients with calcific AS, there were significant differences among the three leaflets (noncoronary, left coronary, and right coronary cusps) in calcification, leaflet thickening, and functional contribution to AS. Calcifications of the noncoronary cusp and the right coronary cusp were shown to contribute more to aortic valve narrowing than the left coronary cusp. However, leaflet thickening unrelated to calcification (fibrosis) was found to more frequently hinder the opening of the left coronary cusp than the other leaflets.
The reasons for the differences in levels of calcium deposit and fibrosis among the leaflets are still not known, although this study suggests that they may be at least partially linked to blood flow patterns around individual valve leaflets. Future studies will need to be done to better understand why there are differences in the disease processes among the leaflets. These results importantly reveal the potential limitation of our current CT-based approach to assessing AS severity solely based on the calcification load of the entire aortic valve. This study emphasizes the need to simultaneously assess fibrosis, in addition to calcification, of individual aortic valve leaflets so that the severity of AS can be more precisely determined to guide the timing of aortic valve replacement.
Other current Stanford-affiliated authors contributing to this study include Sachin Malik, Tie Liang, Andrew Chang, Nazish Sayed, and Philip Tsao.
Ian Chen, MD, PhD